-
-
-
Jakarta, Indonesia
Understanding Stunted Children: Chronic Growth Failure, Early-Life Risks, and Why It Matters Beyond Height
Acute Mesenteric Ischemia: A Vascular Emergency That Requires Immediate Recognition
-
 Post By
Post By -
Published
May 8, 2026
Acute mesenteric ischemia is one of the most dangerous causes of acute abdominal pain in modern emergency medicine. Although less common than many other abdominal emergencies, it carries an exceptionally high risk of bowel infarction, sepsis, multi-organ failure, and death when diagnosis is delayed. The condition occurs when intestinal blood flow falls to a level that is insufficient to meet metabolic demands, leading first to ischemic injury and, if uncorrected, to irreversible transmural necrosis. In practical clinical terms, acute mesenteric ischemia is a race against time: survival depends on rapid suspicion, rapid imaging, and rapid restoration of perfusion when salvageable bowel remains.
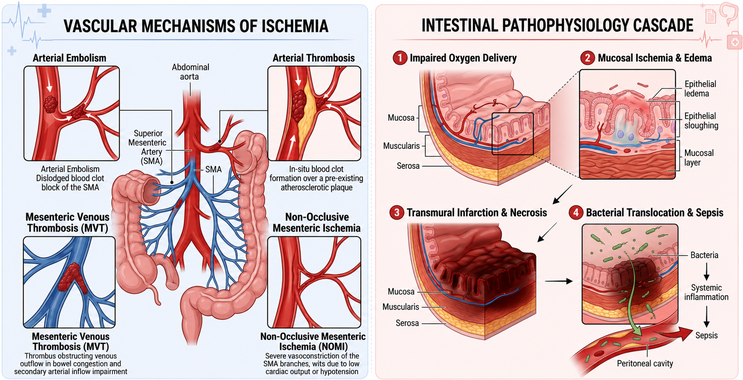
The pathophysiology of acute mesenteric ischemia is heterogeneous. Classically, the condition is divided into four major mechanisms: arterial embolism, arterial thrombosis, mesenteric venous thrombosis, and non-occlusive mesenteric ischemia. Each pathway leads to impaired intestinal oxygen delivery, but the underlying biology and clinical context differ. Arterial embolism often occurs suddenly, frequently in patients with atrial fibrillation or other cardioembolic sources, and may present dramatically with abrupt severe pain. Arterial thrombosis tends to occur on a background of chronic atherosclerotic disease and may be preceded by symptoms of chronic mesenteric ischemia. Mesenteric venous thrombosis impairs venous outflow, causing bowel wall edema, rising capillary pressure, reduced arterial inflow, and eventual ischemic injury. Non-occlusive mesenteric ischemia, by contrast, reflects severe splanchnic hypoperfusion and vasoconstriction, often in critically ill patients with shock, vasopressor exposure, or low-flow states.
One of the reasons acute mesenteric ischemia remains so lethal is that early diagnosis is often difficult. The classic teaching of pain out of proportion to physical findings remains clinically useful, but it is not universally present and should not be treated as a rigid rule. Patients may initially present with severe abdominal pain, nausea, vomiting, diarrhea, or mild abdominal distension, while examination findings remain limited. As ischemia progresses, however, the clinical picture may shift toward peritonitis, metabolic acidosis, hemodynamic instability, and systemic inflammatory response. By that stage, extensive bowel injury may already have occurred. The disease is therefore dangerous not because it is impossible to recognize, but because it is too easy to underestimate during its earlier window.
Current evidence and modern guidelines emphasize the importance of rapid computed tomography angiography in suspected acute mesenteric ischemia. CTA has become the diagnostic imaging modality of choice because it can identify arterial occlusion, mesenteric venous thrombosis, bowel wall abnormalities, reduced enhancement, pneumatosis intestinalis, portal venous gas, and other signs of advanced ischemic injury. Equally important, it can help distinguish mesenteric ischemia from other causes of acute abdomen. Laboratory markers, including leukocytosis, lactate elevation, and metabolic acidosis, may support suspicion but are not sufficiently sensitive to exclude the diagnosis early. A normal early lactate level should never provide false reassurance when the clinical context remains concerning.
Management depends on the mechanism and stage of disease, but several principles are consistent across cases. Initial treatment includes aggressive resuscitation, hemodynamic optimization, broad-spectrum antibiotics when bowel injury is suspected, and urgent consultation with surgery and vascular or endovascular teams. Revascularization is central in occlusive arterial disease when viable bowel remains. In recent years, endovascular approaches have gained increasing importance in selected patients, especially when diagnosis is made before advanced necrosis. Nevertheless, open surgery remains essential when there is concern for bowel infarction, perforation, or peritonitis, because direct assessment of bowel viability and resection of necrotic segments may be life-saving. Mesenteric venous thrombosis may often be treated primarily with anticoagulation, provided that transmural infarction has not already occurred.
The biological consequences of delay are profound. The intestine has high metabolic demand and limited tolerance for sustained hypoperfusion. Ongoing ischemia disrupts mucosal integrity, increases epithelial permeability, promotes bacterial translocation, and triggers systemic inflammatory cascades. Once necrosis develops, the clinical trajectory can deteriorate rapidly into septic shock and multi-organ dysfunction. This sequence explains why acute mesenteric ischemia is not merely a vascular problem of the bowel, but a whole-body critical illness when diagnosis is missed.
Risk stratification is therefore essential. Clinicians should maintain a high index of suspicion in older patients, individuals with atrial fibrillation, diffuse atherosclerotic disease, heart failure, hypercoagulable states, recent low-flow shock, vasopressor dependence, or prior thromboembolic history. Likewise, mesenteric ischemia should remain in the differential diagnosis when abdominal pain appears unusually severe, unexplained, or inconsistent with early examination findings. In emergency medicine, some of the most lethal diagnoses are not those that present loudly, but those that present deceptively.
For the broader public, the key lesson is that severe sudden abdominal pain should never be dismissed, especially in older adults or people with cardiovascular disease. Although acute mesenteric ischemia is less widely known than stroke or myocardial infarction, it shares the same central principle: blood flow loss causes tissue death, and time to treatment matters enormously. Earlier imaging, earlier diagnosis, and earlier intervention offer the best chance to preserve bowel, prevent sepsis, and improve survival.
In conclusion, acute mesenteric ischemia is a vascular emergency with high mortality precisely because diagnosis is often delayed until intestinal injury becomes advanced. The condition demands rapid clinical suspicion, urgent CTA-based evaluation, and prompt mechanism-specific treatment. In both emergency care and public health awareness, the message is clear: unexplained severe abdominal pain—especially in high-risk patients—must be treated with urgency, because delay can mean irreversible bowel loss and death.
References :
1. Clair DG, Beach JM. Mesenteric Ischemia. N Engl J Med. 2016;374:959-968. doi:10.1056/NEJMra1503884.
2. Bala M, Kashuk J, Moore EE, et al. Acute mesenteric ischemia: guidelines of the World Society of Emergency Surgery. World J Emerg Surg. 2017;12:38. doi:10.1186/s13017-017-0150-5.
3. Tilsed JVT, Casamassima A, Kurihara H, et al. ESTES guidelines: acute mesenteric ischaemia. Eur J Trauma Emerg Surg. 2016;42(2):253-270. doi:10.1007/s00068-016-0634-0.
4. Schoots IG, Koffeman GI, Legemate DA, Levi M, van Gulik TM. Systematic review of survival after acute mesenteric ischaemia according to disease aetiology. Br J Surg. 2004;91(1):17-27. doi:10.1002/bjs.4459.
5. Acosta S. Epidemiology of mesenteric vascular disease: clinical implications. Semin Vasc Surg. 2010;23(1):4-8. doi:10.1053/j.semvascsurg.2009.12.001.
6. Oldenburg WA, Lau LL, Rodenberg TJ, Edmonds HJ, Burger CD. Acute mesenteric ischemia: a clinical review. Arch Intern Med. 2004;164(10):1054-1062. doi:10.1001/archinte.164.10.1054.
7. Kärkkäinen JM, Lehtimäki TT, Manninen H, Paajanen H. Acute mesenteric ischemia is a more common cause than expected of acute abdomen in the elderly. J Gastrointest Surg. 2015;19(8):1407-1414. doi:10.1007/s11605-015-2830-3.
8. Ahmed M. Acute mesenteric ischemia: advances in diagnosis and endovascular management. Semin Vasc Surg. 2010;23(1):9-14. doi:10.1053/j.semvascsurg.2009.12.002.
9. Treska V, Certik B, Molacek J, et al. Acute mesenteric ischemia—current diagnostics and therapy. Rozhl Chir. 2020;99(2):54-60.
10. Kärkkäinen JM, Acosta S. Acute mesenteric ischemia (part I) – Incidence, etiologies, and how to improve early diagnosis. Best Pract Res Clin Gastroenterol. 2017;31(1):15-25. doi:10.1016/j.bpg.2016.10.018.
11. Acosta S, Björck M. Modern treatment of acute mesenteric ischaemia. Br J Surg. 2014;101(1):e100-e108. doi:10.1002/bjs.9368.
12. van den Heijkant TC, Aerts BA, Teijink JA, et al. Challenges in diagnosing mesenteric ischemia. World J Gastroenterol. 2013;19(9):1338-1341. doi:10.3748/wjg.v19.i9.1338.
The pathophysiology of acute mesenteric ischemia is heterogeneous. Classically, the condition is divided into four major mechanisms: arterial embolism, arterial thrombosis, mesenteric venous thrombosis, and non-occlusive mesenteric ischemia. Each pathway leads to impaired intestinal oxygen delivery, but the underlying biology and clinical context differ. Arterial embolism often occurs suddenly, frequently in patients with atrial fibrillation or other cardioembolic sources, and may present dramatically with abrupt severe pain. Arterial thrombosis tends to occur on a background of chronic atherosclerotic disease and may be preceded by symptoms of chronic mesenteric ischemia. Mesenteric venous thrombosis impairs venous outflow, causing bowel wall edema, rising capillary pressure, reduced arterial inflow, and eventual ischemic injury. Non-occlusive mesenteric ischemia, by contrast, reflects severe splanchnic hypoperfusion and vasoconstriction, often in critically ill patients with shock, vasopressor exposure, or low-flow states.
One of the reasons acute mesenteric ischemia remains so lethal is that early diagnosis is often difficult. The classic teaching of pain out of proportion to physical findings remains clinically useful, but it is not universally present and should not be treated as a rigid rule. Patients may initially present with severe abdominal pain, nausea, vomiting, diarrhea, or mild abdominal distension, while examination findings remain limited. As ischemia progresses, however, the clinical picture may shift toward peritonitis, metabolic acidosis, hemodynamic instability, and systemic inflammatory response. By that stage, extensive bowel injury may already have occurred. The disease is therefore dangerous not because it is impossible to recognize, but because it is too easy to underestimate during its earlier window.
Current evidence and modern guidelines emphasize the importance of rapid computed tomography angiography in suspected acute mesenteric ischemia. CTA has become the diagnostic imaging modality of choice because it can identify arterial occlusion, mesenteric venous thrombosis, bowel wall abnormalities, reduced enhancement, pneumatosis intestinalis, portal venous gas, and other signs of advanced ischemic injury. Equally important, it can help distinguish mesenteric ischemia from other causes of acute abdomen. Laboratory markers, including leukocytosis, lactate elevation, and metabolic acidosis, may support suspicion but are not sufficiently sensitive to exclude the diagnosis early. A normal early lactate level should never provide false reassurance when the clinical context remains concerning.
Management depends on the mechanism and stage of disease, but several principles are consistent across cases. Initial treatment includes aggressive resuscitation, hemodynamic optimization, broad-spectrum antibiotics when bowel injury is suspected, and urgent consultation with surgery and vascular or endovascular teams. Revascularization is central in occlusive arterial disease when viable bowel remains. In recent years, endovascular approaches have gained increasing importance in selected patients, especially when diagnosis is made before advanced necrosis. Nevertheless, open surgery remains essential when there is concern for bowel infarction, perforation, or peritonitis, because direct assessment of bowel viability and resection of necrotic segments may be life-saving. Mesenteric venous thrombosis may often be treated primarily with anticoagulation, provided that transmural infarction has not already occurred.
The biological consequences of delay are profound. The intestine has high metabolic demand and limited tolerance for sustained hypoperfusion. Ongoing ischemia disrupts mucosal integrity, increases epithelial permeability, promotes bacterial translocation, and triggers systemic inflammatory cascades. Once necrosis develops, the clinical trajectory can deteriorate rapidly into septic shock and multi-organ dysfunction. This sequence explains why acute mesenteric ischemia is not merely a vascular problem of the bowel, but a whole-body critical illness when diagnosis is missed.
Risk stratification is therefore essential. Clinicians should maintain a high index of suspicion in older patients, individuals with atrial fibrillation, diffuse atherosclerotic disease, heart failure, hypercoagulable states, recent low-flow shock, vasopressor dependence, or prior thromboembolic history. Likewise, mesenteric ischemia should remain in the differential diagnosis when abdominal pain appears unusually severe, unexplained, or inconsistent with early examination findings. In emergency medicine, some of the most lethal diagnoses are not those that present loudly, but those that present deceptively.
For the broader public, the key lesson is that severe sudden abdominal pain should never be dismissed, especially in older adults or people with cardiovascular disease. Although acute mesenteric ischemia is less widely known than stroke or myocardial infarction, it shares the same central principle: blood flow loss causes tissue death, and time to treatment matters enormously. Earlier imaging, earlier diagnosis, and earlier intervention offer the best chance to preserve bowel, prevent sepsis, and improve survival.
In conclusion, acute mesenteric ischemia is a vascular emergency with high mortality precisely because diagnosis is often delayed until intestinal injury becomes advanced. The condition demands rapid clinical suspicion, urgent CTA-based evaluation, and prompt mechanism-specific treatment. In both emergency care and public health awareness, the message is clear: unexplained severe abdominal pain—especially in high-risk patients—must be treated with urgency, because delay can mean irreversible bowel loss and death.
References :
1. Clair DG, Beach JM. Mesenteric Ischemia. N Engl J Med. 2016;374:959-968. doi:10.1056/NEJMra1503884.
2. Bala M, Kashuk J, Moore EE, et al. Acute mesenteric ischemia: guidelines of the World Society of Emergency Surgery. World J Emerg Surg. 2017;12:38. doi:10.1186/s13017-017-0150-5.
3. Tilsed JVT, Casamassima A, Kurihara H, et al. ESTES guidelines: acute mesenteric ischaemia. Eur J Trauma Emerg Surg. 2016;42(2):253-270. doi:10.1007/s00068-016-0634-0.
4. Schoots IG, Koffeman GI, Legemate DA, Levi M, van Gulik TM. Systematic review of survival after acute mesenteric ischaemia according to disease aetiology. Br J Surg. 2004;91(1):17-27. doi:10.1002/bjs.4459.
5. Acosta S. Epidemiology of mesenteric vascular disease: clinical implications. Semin Vasc Surg. 2010;23(1):4-8. doi:10.1053/j.semvascsurg.2009.12.001.
6. Oldenburg WA, Lau LL, Rodenberg TJ, Edmonds HJ, Burger CD. Acute mesenteric ischemia: a clinical review. Arch Intern Med. 2004;164(10):1054-1062. doi:10.1001/archinte.164.10.1054.
7. Kärkkäinen JM, Lehtimäki TT, Manninen H, Paajanen H. Acute mesenteric ischemia is a more common cause than expected of acute abdomen in the elderly. J Gastrointest Surg. 2015;19(8):1407-1414. doi:10.1007/s11605-015-2830-3.
8. Ahmed M. Acute mesenteric ischemia: advances in diagnosis and endovascular management. Semin Vasc Surg. 2010;23(1):9-14. doi:10.1053/j.semvascsurg.2009.12.002.
9. Treska V, Certik B, Molacek J, et al. Acute mesenteric ischemia—current diagnostics and therapy. Rozhl Chir. 2020;99(2):54-60.
10. Kärkkäinen JM, Acosta S. Acute mesenteric ischemia (part I) – Incidence, etiologies, and how to improve early diagnosis. Best Pract Res Clin Gastroenterol. 2017;31(1):15-25. doi:10.1016/j.bpg.2016.10.018.
11. Acosta S, Björck M. Modern treatment of acute mesenteric ischaemia. Br J Surg. 2014;101(1):e100-e108. doi:10.1002/bjs.9368.
12. van den Heijkant TC, Aerts BA, Teijink JA, et al. Challenges in diagnosing mesenteric ischemia. World J Gastroenterol. 2013;19(9):1338-1341. doi:10.3748/wjg.v19.i9.1338.

Urinary Tract Infection Updates: Current Clinical and Public Health Developments
Urinary tract infection remains one of the most common bacterial infections globally, with current updates focusing on antimicrobial resistance, diagnostic stewardship, recurrent infection management, catheter-associated prevention, and emerging non-antibiotic strategies. This article reviews recent developments relevant to clinicians, researchers, and public health professionals.
Top 5 Vegetables That May Enhance Immune Function: An Evidence-Based Nutritional Overview
Dietary patterns rich in vegetables are consistently associated with improved health outcomes, including support of normal immune function. This article reviews five vegetables—broccoli, spinach, garlic, carrots, and red bell peppers—that may contribute to immune resilience through their content of vitamins, minerals, antioxidants, and bioactive phytochemicals.


Understanding Stunted Children: Chronic Growth Failure, Early-Life Risks, and Why It Matters Beyond Height
Stunting in children refers to impaired linear growth resulting from chronic undernutrition, repeated infection, and unfavorable early-life conditions. More than a matter of short stature, stunting reflects a broader process of biological and developmental disadvantage that can affect cognitive outcomes, school performance, and long-term health.
Blood Pressure Monitoring as a Public Health Priority: Strengthening Early Detection and Long-Term Cardiovascular Prevention
Blood pressure monitoring remains one of the most practical and impactful tools in public health for identifying hypertension early, guiding treatment decisions, and reducing long-term cardiovascular risk. Wider adoption of accurate office, community, and home-based monitoring strategies could significantly improve prevention of stroke, heart disease, kidney damage, and premature mortality.

